
Insights from a pilot survey of Ontario medical office administrators
EXECUTIVE OVERVIEW
Three drivers of unproductive call volume in medical clinics
We surveyed 30 medical office administrators at Ontario-based clinics about the issues patients most often call about.
Results highlighted three common friction points that drive unproductive call volume and unnecessarily increase pressure on administrative staff:
📅 Appointment logistics and communication gaps.
📞 Avoidable “clinical follow-through” calls.
🗂️ Paperwork and billing inquiries are a significant volume driver (often underestimated).
What does this mean for automation readiness?
The results suggest many requests are repetitive, predictable, and driven by process gaps—ideal candidates for automation in principle.
However, the systems behind these requests are fragmented, so workflows must be standardized, and communication tools integrated, before many tasks can be automated.
HIGH IMPACT FIXES that can be implemented quickly and at little/no cost:
☎️ Implement consistent call structure and call handling standards to reduce uncertainty, better manage patients’ expectations, and reduce miscommunication.
ℹ️ Establish consistent and easily accessible information sources for patients for routine questions.
High-impact fixes that can be implemented within 2-4 months through communication system upgrades and streamlining workflows:
🔗 Integrating communication pathways (e.g. calls, messages, faxes, etc.) for increased visibility, documentation, and control.
⏰ Improved appointment reminders and appointment confirmation functions.
📣 Predictable status and results communication pathway.
📝 Improved tools to support repetitive tasks (e.g. intake forms, refill checklists, form/note templates, etc.).
Freeing staff to address challenging and exceptional cases and advancing care
Unproductive call volume takes time away from productive work, including creating new care opportunities, supporting advanced care, and improving access to care, especially for patients requiring additional support.
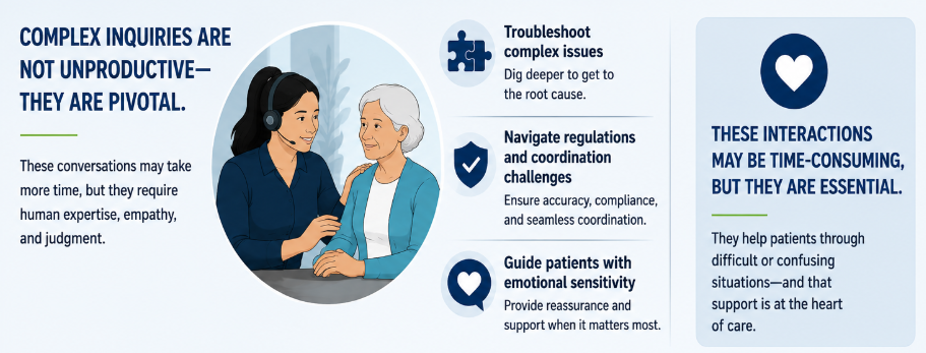
Some inquiries require administrative staff to take time to troubleshoot complex issues, navigate health regulations and coordination challenges, and guide patients through their healthcare journey with emotional sensitivity. These, more challenging, interactions can be time-consuming but should not be confused for unproductive. In fact, they are often pivotal in supporting patients facing difficult or confusing situations.
REPORT
Introduction
The healthcare space is flooded with AI and automation options, with administrative phone calls often pitched as the first “low hanging fruit”. In practice, many projects, particularly in small and medium-sized clinics, get stalled or abandoned. Reasons range from weak ROI to lack of trust. Another prominent issue is workflow disruption, especially when technology is introduced without a clear goal or demonstrated ability to solve a specific problem.
To truly serve patients and healthcare professionals, technological solutions must be grounded in the realities of daily clinic workflows and address real friction points. To begin building this understanding, we surveyed 30 medical administration professionals from Ontario clinics to:
(1) identify the common drivers of unproductive call volume,
(2) pinpoint common workflow pain points, and
(3) inform strategies for system streamlining and automation.
What do patients call about?
Despite the growing prevalence of self-serve booking systems[1], most patient phone calls are about booking appointments. In specialist clinics, where patients are booked by referral, many calls are about appointment coordination, date changes, and other aspects of appointment management, which can be complex when testing procedures and multiple healthcare providers are involved.
“Unproductive call volume reflects system design, not patient demand.”
What is “unproductive call volume”?
Calls can be categorized as:
✅ Productive (creates new patient care)
⚠️ Necessary support (complex / human-needed/ advance patient care)
❌ Unproductive (preventable)
Unproductive call volume refers to calls that do not create new value, but instead compensate for something that should have already happened or been communicated. In other words, these are calls generated by broken or invisible workflows – not real demand.
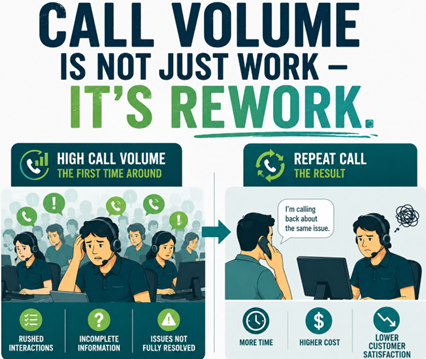
Status-chasing and premature follow-up calls
These calls happen when status is invisible, not communicated, or misaligned with patients’ expectations. For example, when patients call for results “too early”, or expect referrals before typical processing time.
These calls are often repeated multiple times for the same issue.

Failure-recovery calls (fixing something that broke)
These calls happen when something went wrong with the original task.
Often as a result of handoff failure and when something was not recorded or communicated properly (e.g. preferred pharmacy was not confirmed). Often trigger duplicate work and rework.

Communication gap calls
These are calls that would have been best handled as outbound calls or text messages. They include appointment reminders and confirmations. These types of calls convert outbound work into inbound call volume, requiring additional time to investigate and resolve the issue each time. They typically happen because of missing outbound communication processes and lack of visibility.

Queue-driven repeat calls
Clinics often have periods of high call volume (e.g. Monday spikes), which result in long hold times and missed callbacks. When patients are left on hold too long, or not called back, they often call again. This amplifies the call volume and often results in duplicated work, such as when a different administrators pick up calls from the same caller, and the caller has to re-state the issue.
Problem! When faced with high unproductive call volume, clinic administrators have less time to deal with productive and necessary support calls. This means less time to support patients and enroll new patients. Patients with new clinical concerns, potentially urgent symptoms, or individuals requiring complex assistance, risk falling through the cracks.
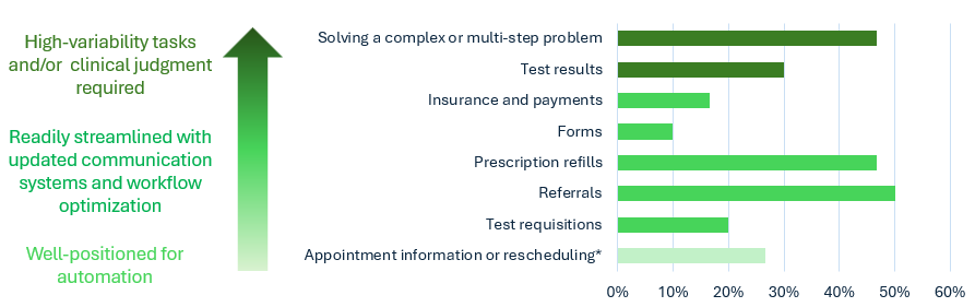
Figure 1: Percentage of survey respondents who identified the issue as frequently called about. (*appointment coordination for some specialist clinics is complex and not easily automatable)
Problem! Unchecked, unreceived, or unprocessed messages result in repeat patient calls and missed appointments.
Tech fix: Updating voicemail to shared-access box, with trackable status, searchable transcription and summaries can streamline workflow and enable task-sharing among staff. This type of simple upgrade can save hours of time, help resolve message backlogs, and reduce unproductive call volume.
Friction Point 1: Appointment logistics and communication gaps
Aside from booking new appointments, a commonly cited reason for calls was appointment information or rescheduling. While some of these calls are necessary, particularly when rescheduling is required (e.g. sooner appointments for symptomatic patients), many responses pointed to communication gaps as an important driver of avoidable calls and/or patient complaints.
The subset of survey responses listed here highlight communication gaps that persist across clinics. They tend to increase call volume, sometimes during already busy periods, while adding little or no value to the patient experience. Common patterns in the responses include missing or incomplete reminder calls, under-communicated appointment or follow-up information, and unmet patient expectations for call-backs. These responses highlight opportunities for several high-impact fixes.
“A lack of communication quickly becomes a loss of trust.”
Sample responses signaling unproductive call volume:
“Wait time and not being called back.”
“Not having their calls returned and long wait times on busy days, especially Mondays.”
“Not being informed when their next appointment is.”
“Patients call to be provided their existing appointment information.”
“Patients call regarding appointment reminders.”
“Patients call because they are not able to confirm their appointment when they get the reminder call.”
[Specialist clinic] “Patients get confirmation calls for only one appointment of multiple.” [Specialist clinic] “Patients get confirmation calls for only one appointment of multiple.”
[Specialist clinic] “Patients call about the specialist plan after they were seen.”
[Virtual appointments] “Patients call when they cannot log into zoom for their virtual appointments.”
High-impact fixes:
- Establish consistent and easily accessible information sources for patients for routine questions and troubleshooting, such as:
- “What to expect” information sheets, especially for specialists
- “Virtual visit tech support” checklist or micro-script
- Upgrade voicemail system to trackable shared-access model with message transcription and summarization.
- Improved appointment reminder systems:
- Implement a consistent reminder system, if one is not in place or suffers from gaps.
- Update reminder systems for handling multiple appointments per patient (where applicable)
In most clinics, all three types of fixes can be implemented within a few weeks and at little up-front cost.
Appointment reminders are, on the whole, highly repetitive and logically uncomplicated. They are one of the easier types of tasks to streamline through tweaks in workflow and upgrades in communication systems. For the same reasons, they are (in principle) highly automatable, assuming that the necessary technological[2] and organizational prerequisites[3] are in place. Automation can serve as a great long-term high-impact fix, but it typically requires greater financial investment and organizational change management.
Friction point 2: Avoidable “clinical follow-through” calls
Avoidable calls about clinical follow-through are another prominent friction point in the survey results. These are calls that are driven by gaps between clinical decisions and administrative execution and/or communication. That is, the care plan exists (e.g. prescription, referral, diagnostic testing, etc.), but something breaks down in the execution and communication of the plan, so that the patients feel that they have to call to “close the loop”.
While some calls are necessary and productive, for example, requesting a new prescription refill or test requisition, others are follow-up calls regarding the same task, or requests for resends.
Problem! Requests for fax resends due to fax not received or fax sent to the wrong number. Faxes are notoriously error-prone (due to manual data entry requirements) and difficult to keep track of. Fax processing can pose significant workflow problems and create bottlenecks in clinical follow-through.
Tech fix: Upgrading fax to a easy-to-use, trackable shared-box model with notes and status updates, will reduce errors, save time on re-sends, and improve data security.
We have identified two reasons for why these unproductive calls happen:
- Delays in administrative processing of referrals, prescriptions, and test requisitions.
- Delays can happen at busy times when admin staff are forced to prioritize urgent calls or issues.
- Even during slower periods, task handling can be significantly slowed by inefficient or outdated communication systems.
- Fax systems are a major culprit. It is not uncommon for tasks to get stuck at the fax processing stage, especially in larger clinics, some of which send and receive hundreds of faxes per day.
- Breakdowns in the communication follow-through. Orders, prescriptions, referrals, forms, and other communications requested by the doctor are usually completed (though sometimes with delay), but there is no consistent confirmation or communication with patients regarding completion.
Inability to see the task status or having a clear timeframe with next steps tends to leave patients anxious, with some patients calling repeatedly for updates or confirmation of task completion. Furthermore, with outdated communication systems, checking status for a patient can be difficult and time-consuming.
High-impact fixes:
- Without rushing to complicated and costly automation projects, many clinics can gain immediate value by upgrading to integrated communication systems (i.e. calls, messages, and faxes, accessible in one place) that enables shared access for increased visibility, documentation, and control.
- Fax upgrades in particular offer a low-cost, high-value fix[4].
- An often overlooked (and underestimated) fix is the establishment of a consistent call structure and call handling standard throughout the organization. For example:
- Ensuring that every call includes a data intake check (e.g. was all of the necessary information gathered to complete the task? Was the pharmacy fax number confirmed?)
- Ensure that by the end of each call, the patient understands the next steps and timelines.
- Ensure that there is complete and accurate documentation for each call.
- Implementing a predictable status and results communication pathway.
- While establishing a consistent (and/or automated) communication pathway may require a significant lift in IT and organizational change management, it will ultimately address the root of most task follow-up calls.
Friction Point 3: Paperwork and billing inquiries are a significant volume driver (often underestimated).
A surprising result from our survey was that billing inquiry calls are a significant driver of call volume, even in Ontario clinics. For example, some callers are unaware that certain services are not covered by OHIP, which can spark worry and confusion for some patients, leading to time spent on routine explanations.
Similarly, calls regarding filling out medical forms, paperwork for insurance and other purposes, and updating records, were more common and more time consuming than we anticipated. This was especially the case with specialist clinics, some of which require completion of lengthy intake forms, which can be difficult to understand for some patients.
While some of the resulting call volume is necessary for advancing patient care, we found that some types of calls can be avoided or significantly shortened with tweaks in workflow and implementation of new tools.
High-impact fixes:
- Developing easily accessible information and help tools can reduce uncertainty for patients, enhance accessibility and transparency, and save time for both the patients and the clinic staff.
- Examples include billing FAQ, accessible price lists for uninsured services, online forms with built-in explanatory notes, and medical note templates.
- Developing automation solutions for repetitive paperwork will address much of the unnecessary call volume stemming from confusion, errors, and difficulty of use. However, for many clinics it would require a significant lift to achieve automation readiness.
CONCLUSION
The findings of this pilot survey point to a consistent theme, that much of the excessive unproductive call volume is driven by: (1) outdated, fragmented communication systems and (2) gaps in workflow consistency and standardization.
Importantly, these issues do not require large-scale, high-cost automation initiatives to address. On the contrary, the data suggests that targeted, high-impact improvements in communication infrastructure and workflow structure can resolve a substantial portion of these gaps.
Upgrades such as shared-access communication tools, trackable voicemail and fax systems, consistent call handling standards, and clearly defined status pathways can dramatically reduce unproductive call volume while improving both patient experience and staff efficiency. These changes are often achievable with modest investment and can be implemented within short timeframes.
At the same time, the report highlights a critical barrier to successful adoption of more advanced automation solutions: many clinics lack the foundational prerequisites required for automation to deliver meaningful value.
In environments where workflows are inconsistent, intake processes are incomplete, and task ownership and status visibility are unclear, automation technologies are likely to amplify existing inefficiencies rather than resolve them. This helps explain why many automation projects fail to meet expectations or generate sustainable ROI.
For clinics to fully benefit from automation, the priority must first be on strengthening system integration and establishing clear, standardized workflows. By building this operational foundation, clinics not only reduce immediate friction and inefficiency, but also position themselves for successful, scalable adoption of automation technologies in the future. In this sense, streamlining and automation should be viewed not as competing approaches, but as sequential steps in a broader strategy to modernize medical office operations and better serve both patients and healthcare providers.
NEXT STEPS
- Quantifying unproductive call volume and impact of streamlining and automation opportunities
- Analyzing technological and organizational readiness for high-impact automation
[1] Implementation of self-serve booking systems face many of the same problems as other types of automation, including fragmented systems, issues with patient experience, and lack of measurable ROI.
[2] Core technological prerequisites for automation include a reliable scheduling system, integration layer (APIs, webhooks), communication infrastructure, preferably with multi-channel delivery, with messaging API, automation engine, and two-way communication capability. For healthcare, a compliance and security layer is non-negotiable.
[3] Automation only works if the underlying workflow is consistent. Process standardization, accountability, change management readiness, communication policies, data and decision governance, are some of the key, and often overlooked, prerequisites for successful process automation.
[4] Some clinics work with expensive, but outdated, fax systems. In these cases an upgrade can actually generate savings.
| Anastasia Hervas | Director of Research, Training, and Compliance Ph.D., M.Sc. Anastasia.hervas@stratovox.com |